ACR
Albuminuria
Albuminuria is increased excretion of urinary albumin and a marker of kidney damage. Normal individuals excrete very small amounts of protein in the urine. Albumin is the most common type of protein in the urine. All patients with CKD should be screened for albuminuria. Persistent increased protein in the urine (two positive tests over 3 or more months) is the principal marker of kidney damage, acting as an early and sensitive marker in many types of kidney disease.
Detecting albuminuria
A routine dipstick is not sensitive enough to detect small amounts of urine protein. Therefore, it is recommended that screening in adults with CKD or at risk for CKD be done by testing for albuminuria.
Albumin-to-creatinine ratio (ACR) is the first method of preference to detect elevated protein. The recommended method to evaluate albuminuria is to measure urinary ACR in a spot urine sample. ACR is calculated by dividing albumin concentration in milligrams by creatinine concentration in grams.
Although the 24-hour collection has been the "gold standard," alternative methods for detecting protein excretion such as urinary albumin-to-creatinine ratio (ACR) correct for variations in urinary concentration due to hydration as well as provide more convenience than timed urine collections. The spot specimen correlates well with 24-hour collections in adults.
Definitions of abnormalities in albumin excretion
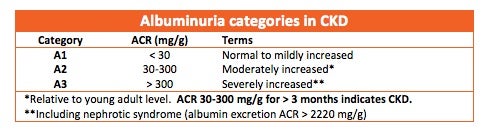
Moderately increased albuminuria, historically known as microalbuminuria, (ACR 30-300 mg/g) refers to albumin excretion above the normal range but below the level of detection by tests for total protein. Severely increased albuminuria, historically known as macroalbuminuria, (ACR >300) refers to a higher elevation of albumin associated with progressive decline in glomerular filtration rate. The following chart lists the albuminuria categories in CKD.